Published guidance, policy, official data, or peer-reviewed evidence carries the claim.
Policy asks
What needs to change
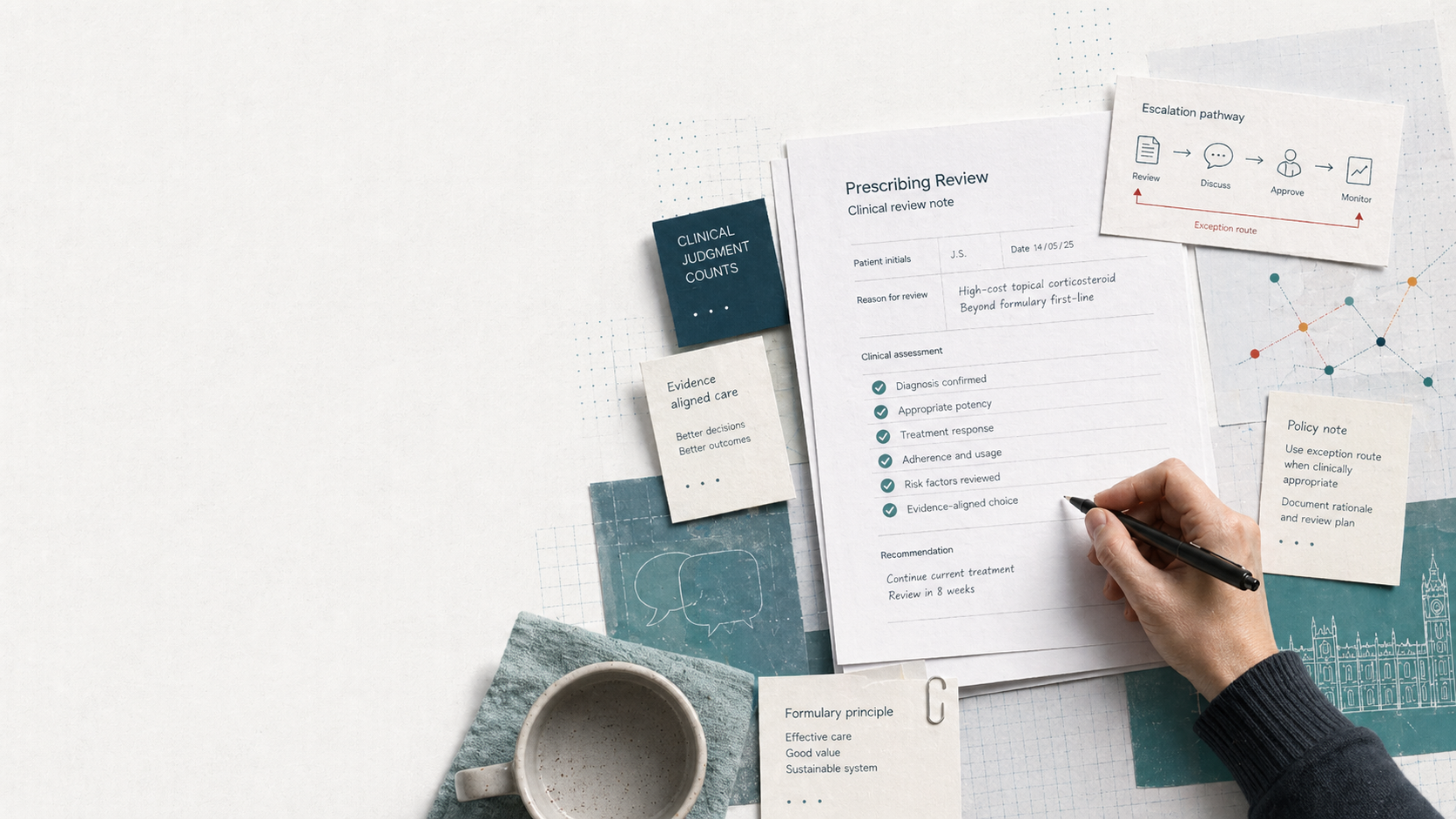
The campaign is not asking for unrestricted prescribing or one preferred product. It is asking for a system that notices when standard options fail, records that failure clearly, and gives clinicians a practical route to prescribe something more suitable.
These asks focus on documented need, prescribing flexibility, total-care assessment, and stronger interim care during long specialist waits.
Evidence key
Each ask carries its evidence footing.
Sourced principles, patient testimony, and citation-required policy questions stay separate.
Lived experience shows how pathways can break down, but it is not treated as clinical proof.
Important claims remain clearly marked until the source trail is verified.
Five asks
Clear, bounded changes for prescribing policy.
Each ask is a campaign recommendation. The underlying principles are source-backed where marked, while the exact policy model and system-cost questions remain citation-required.
- Policy recommendation
Recognise documented emollient failure as a reason to review prescribing options.
A record of poor tolerance, non-use, or inadequate response should trigger a practical review rather than repeated cycling through unsuitable first-line products.
Evidence footing: sourced principle on emollient choice and acceptability; campaign recommendation on the prescribing review route.
- Policy recommendation
Give GPs clearer routes to prescribe clinically suitable alternatives when formulary options fail.
Primary care needs a defined route for justified exceptions before a patient has waited for specialist review.
Evidence footing: campaign recommendation based on sourced prescribing principles and citation-required pathway evidence.
- Policy recommendation
Assess eczema prescribing by total care cost, not only unit product cost.
Decision-makers should test whether acquisition-cost savings are offset by repeat demand, escalation, referral pressure, or self-funded care.
Evidence footing: campaign recommendation; cost scale and model claims remain citation-required.
- Requires policy review
Review whether selected fragrance-free, paraffin-free, or otherwise clinically appropriate alternatives should be available for documented need.
This is a targeted review request, not a recommendation for any named product or an argument for unrestricted prescribing.
Evidence footing: campaign recommendation; product-specific, ingredient-specific, and mechanism claims remain citation-required.
- Policy recommendation
Treat long dermatology waits as a reason to strengthen primary-care eczema management, not defer it.
Interim care may be the practical NHS pathway for many months, so first-line failure needs a clearer response.
Evidence footing: campaign recommendation; current waiting-time and system-cost data remain citation-required.
Boundary
Cost discipline and clinical suitability can coexist.
The campaign is asking decision-makers to measure the right cost and act on documented failure.
Next step
The next step is scrutiny of the route after first-line failure.
Decision-makers can use the asks to review how documented emollient failure is recorded, escalated, and assessed against total care cost.